A recent article from the April edition of American Academy of Orthopaedic Surgeons focused on how hip injuries can lead to long-term negative effects within the athletic community. To thoroughly explain how these injuries occur, the authors Dean Lynch, Aseesh Bedi, and Christopher Larson discuss the hip joint according to four separate layers.
The Osseous Layer
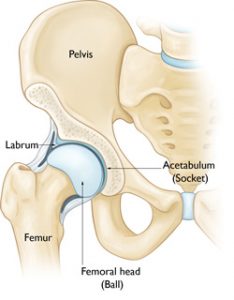
The first layer involves the femur bone, the pelvis and the hip socket. Hip injuries to this layer often include:
-
Static overload
-
Impingement
-
Dynamic instability
Another less common hip injury is femoroacetabular impingement, or FAI. FAI is a condition that limits range of motion in the hip because of improper bone formation during childhood. The decrease in movement within the hip causes abnormal stress to the sacroiliac joint, pubic symphysis, and lumbar spine. Cam impingement is one variety of FAI where the femoral head is not round and therefore cannot rotate smoothly inside the acetabulum. A bump forms on the edge of the femoral head that grinds the cartilage inside the acetabulum. Also, if an anterior cam effect is present it can limit internal rotation. So it may cause levering of the femoral head which could also create posterior hip subluxation or dislocation and resultant labral tearing and cartilage damage.
The Capsuloligamentous Layer
This layer includes:
-
Labrum
-
Joint capsule
-
Ligamentum/capular complex
-
Ligamentous teres
Asymmetric wear of the chondral surfaces of the femoral head and/or the acetabulum may result from stress of the Osseous layer. The authors noted in their study that the structure of layer one produces an injury pattern for the second layer. For example, if an athlete has FAI and hip pain then a labral tear is highly likely.
The Myotendinous Layer
Layer three includes all the muscles around the pelvis, lumbosacral and pelvic floor regions. Dynamic impingement from a cam deformity in layer one causes increased strain on the SI joints, pubic symphysis and ischium. Secondary strain is placed on muscles attached around the hip joint. Due to the increased strain of the muscles and tendons it can cause tendinitis of enthesopathies.
The Neurokinetic Layer
Layer four includes the nerves within the hip area:
-
Thoracolumbosacral plexus
-
Lumbo pelvic tissues
-
Ilio inguinal
-
Iliohypogastric
-
Genitofemoral
The Neurokinetic layer is responsible for the posture and the ability to sense stimuli of the pelvis over the femur.
Athletic Hip Injuries
Common hip injuries for athletes include:
Adductor Strains
Specific muscles contribute to adductor strains. These muscles include: the adductor longus, adductor magnus, adductor brevis, gracilis, obturator externus and pectineus. The adductor longus is the most common muscle to sustain injury. On average, a soccer player with a strained adductor longus will lose 2 weeks of play time, and will have a 18 percent recurrence rate. It is important to take time to heal because player who return to practice too quickly will likely worsen their injury.

Osteitis pubis
This condition occurs from overuse and stress of the pubis symphysis. It can cause lower abdominal pain secondary to stress and abnormal motion of the joint. The rectus abdomens elevates the pubic bone and the adductor tensions depress the pubic bone. An imbalance can cause a stress injury to the pubic bone. Chronic pubic symphysis can cause chronic sclerosis and widening of the symphysis. The best imaging for diagnosis of the condition is a MRI.
Athletic pubalgia/core muscle injury
Athletic pubalgia/core muscle injury is commonly referred to as a sports hernia. There is no actual hernia associated with the condition, rather it’s more of a weakening or tearing of the abdominal wall. The pain radiates into the groin and proximal adductors during sporting activities. Pain will be reproduced with a resisted setup, palliation over the pubis and the abdominal obliques and or rectus abdominus. Most imaging studies will be normal. On occasion an MRI can pick up a thinning of the abdominal wall or a tear called a cleft sign. Management is done through activity modification, NSAIDS and physical therapy. Sometimes injections will help diagnosis and treat the condition. Sports hernias rarely resolve without surgical intervention. Surgical procedures fall under three classes. These classes include: open repair with or without mesh, scope repair, pelvic floor repair with or without adductor release/repair and neurectomy.
Dr. Stacie Grossfeld is a double board-certified orthopedic surgeon in Louisville, KY with a specialty in sports medicine. If you are suffering from hip pain that is not going away or you have injured your hip and need medical attention from an experienced orthopedic doctor, contact Dr. Grossfeld today by calling 502-212-2663.
Recent Comments