
Inflammation is your body’s natural response to injury or illness, but chronic inflammation can contribute to various health problems. One way to combat chronic inflammation is by adopting a diet rich in non-inflammatory foods. In this article, we’ll explore a list of non-inflammatory foods that can help promote overall health and well-being.
1. Fatty Fish
Fatty fish like salmon, mackerel, and sardines are abundant sources of omega-3 fatty acids, which have potent anti-inflammatory properties. These essential fats help reduce inflammation throughout the body and are excellent for heart and brain health.
2. Leafy Greens
Leafy greens such as spinach, kale, and Swiss chard are packed with vitamins, minerals, and antioxidants. They are low in calories and high in fiber, making them ideal choices for an anti-inflammatory diet.
3. Berries
Blueberries, strawberries, raspberries, and blackberries are bursting with antioxidants that combat inflammation. They are also rich in vitamins and fiber, making them a delicious and nutritious addition to your diet.
4. Turmeric
Turmeric is a spice known for its potent anti-inflammatory compound called curcumin. Adding turmeric to your meals or drinking turmeric tea can help reduce inflammation and may alleviate symptoms in conditions like arthritis.
5. Ginger
Ginger is another spice with anti-inflammatory properties. It can be used fresh or in powdered form and is often included in teas, soups, and stir-fries.
6. Nuts and Seeds
Almonds, walnuts, flaxseeds, and chia seeds are excellent sources of healthy fats, fiber, and antioxidants. They not only help combat inflammation but also support heart health.
7. Olive Oil
Extra virgin olive oil contains monounsaturated fats and antioxidants that can help reduce inflammation and protect against chronic diseases. Use it as a salad dressing or for light sautéing.
8. Cruciferous Vegetables
Broccoli, cauliflower, Brussels sprouts, and cabbage belong to the cruciferous vegetable family. They are rich in sulfur-containing compounds that support the body’s natural detoxification processes and have anti-inflammatory effects.
9. Tomatoes
Tomatoes are a great source of lycopene, an antioxidant known for its anti-inflammatory properties. Cooking tomatoes can enhance the absorption of lycopene, so enjoy them in sauces and stews.
10. Green Tea
Green tea is packed with polyphenols, which have anti-inflammatory and antioxidant effects. Sipping on green tea regularly can be a soothing and health-promoting habit.
11. Whole Grains
Opt for whole grains like brown rice, quinoa, and oats instead of refined grains. Whole grains provide fiber and nutrients that help regulate blood sugar and reduce inflammation.
12. Lean Protein
Lean sources of protein such as skinless poultry, tofu, and legumes are essential for muscle repair and overall health. They provide protein without the pro-inflammatory saturated fats found in red meat.
Conclusion
Incorporating non-inflammatory foods into your diet is a proactive approach to promoting your health and well-being. By choosing foods rich in antioxidants, omega-3 fatty acids, and anti-inflammatory compounds, you can help your body combat chronic inflammation and reduce the risk of various health conditions. Remember that a balanced diet, regular exercise, and a healthy lifestyle are key components of overall wellness, so strive for a well-rounded approach to a healthier you!
If you or someone you love suffers from an inflammatory condition in the Louisville, Kentucky-area, board certified sports medicine physician Dr. Stacie Grossfeld at Orthopaedic Specialists PLLC can help. Orthopaedic Specialists PLLC is accepting new patients, and same day appointments are available. For additional information or to schedule an appointment, please contact Orthopaedic Specialists PLLC today at 502-212-2663.

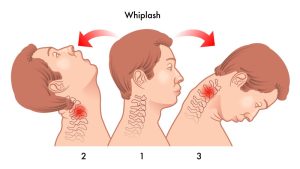 This type of injury is known by terms other than whiplash, such as neck strain or neck sprain, so it might be called by a different name when it comes to articles on the internet or health providers. It also refers to a broader range of injuries rather than just one, like most other injury-related terms do, because when the neck bounces back and forth, the muscles, ligaments and tendons, and/or joints are manipulated past the point of their normal range of motion.
This type of injury is known by terms other than whiplash, such as neck strain or neck sprain, so it might be called by a different name when it comes to articles on the internet or health providers. It also refers to a broader range of injuries rather than just one, like most other injury-related terms do, because when the neck bounces back and forth, the muscles, ligaments and tendons, and/or joints are manipulated past the point of their normal range of motion.




Recent Comments