The Effects of Fitness on the Aging Process
As we age, are there patterns of physical decline? Can those be slowed down or reversed with change in lifestyle? An excellent article was published in the September 2014 volume of the Journal of American Academy of Orthopedic Surgeons. Dr. Bryan Vopat discussed the common physical changes that occur with aging and how to slow down this decline with physical training. A summary of the article is below.
The major changes that occur in the musculoskeletal system with aging are: bone density loss (osteoporosis), the strength and flexibility of muscles decrease (sarcopenia), ligaments and tendons become stiffer and articular cartilage that covers the ends of bones breaks down (osteoarthritis).
Aging Athletes Competing Longer and Performing Better
Evidence over recent years has documented that older athletes are competing longer, and better then they have in the past. They are competing with younger athletes and breaking records within their age groups. These trends are changing the way we think about the older athlete and physical aging.
Older athletes are role models for the concept that age-related decline is not inevitable and that physical activity can counteract the decline in muscle loss, bone loss, and reduced flexibility. More and more athletes are competing in marathon and ironman triathlete events. At the Ironman Triathlon, the number of athletes older than 40-years-old has increased from 25 percent to 50 per cent over the last 25 years! While the number of marathon runners over age 40 has increased over the last 20-30 years, making 50 percent of all marathons older than 40-years-old.
cent over the last 25 years! While the number of marathon runners over age 40 has increased over the last 20-30 years, making 50 percent of all marathons older than 40-years-old.
Eight masters (older than age 40) Ironman Triathlon records were set in 2010 with three of the records set in the age group of 65 years and up. For the past 25 years at ironman events, the average performance has improved by 7.5 percent for all age groups older than 45-years-old.
A study that looked at 900,000 marathon runners found that 25 percent are in their mid to late 60s and outperformed half of the runners age 20-54. One of the most interesting findings from the article is the results from the New York City Marathons from 1989 to 2009. This research found that the running times for men older than 64 and women older than 44 years have not yet plateaued. They are constantly improving with the athletes getting faster. This indicates that they have not likely reached their performance limits.
Aging and Bone Loss
Typically women start losing bone mass at age 30 and can lose up to 1 percent per year. After menopause, that percentage rises to 3 percent per year. Men, on the other hand, begin losing bone mass much later. Starting at age 40, men lose bone mass at a slow rate of 0.5 percent per year and that does not accelerate until they reach their 70s and 80s.
Research has shown that exercise can prevent bone loss in the older athlete. A study examining master sprinters, ages ranging from 40-85 years old, maintained tibial bone strength and bone density. Senior Olympic runners over age 65 had significantly greater overall bone mineral density numbers compared to controls. They also found that when comparing the senior Olympic runners to senior Olympic swimmers, the runners had better bone mineral density indicating that weight bearing exercise is critical.
In the seniors who participated in tai chi for 6 months had increased scores (6-9 %) on their bone density DEXA scans, compared to inactive women in their age group. This indicates that some exercise is better than none and that exercise doesn’t have to be performed at a competitive level.
(more…)
 physician Dr. Stacie Grossfeld enjoys providing training to people in the medical field through her medical practice Orthopaedic Specialists. Over the years, Dr. Grossfeld has offered training opportunities for many physicians interested in learning more about sports medicine, orthopedics and orthopedic surgery. She also mentors college students who are considering pursuing a career in medicine.
physician Dr. Stacie Grossfeld enjoys providing training to people in the medical field through her medical practice Orthopaedic Specialists. Over the years, Dr. Grossfeld has offered training opportunities for many physicians interested in learning more about sports medicine, orthopedics and orthopedic surgery. She also mentors college students who are considering pursuing a career in medicine. Memorial University in Harrogate, Tennessee. Reflecting on the orthopedic and sports medicine training that she received with Dr. Grossfeld at Orthopaedic Specialists, Allyson states:
Memorial University in Harrogate, Tennessee. Reflecting on the orthopedic and sports medicine training that she received with Dr. Grossfeld at Orthopaedic Specialists, Allyson states: orthopedics and sports medicine grow immensely. Dr. Grossfeld is a great doctor, surgeon, teacher and mentor. With the knowledge and skills she has instilled in me, I hope I can continue with a future in orthopedics and provide care for my patients the way that she has taught me.” (more…)
orthopedics and sports medicine grow immensely. Dr. Grossfeld is a great doctor, surgeon, teacher and mentor. With the knowledge and skills she has instilled in me, I hope I can continue with a future in orthopedics and provide care for my patients the way that she has taught me.” (more…)
 useful for daily medical emergencies, or even extreme scenarios. By offering step-by-step instructions during any emergency, this app becomes remarkably useful. There are videos and animations that describe in detail ways to provide care until emergency responders are able to take over. This app can also become a way for you to test your first aid skills before an emergency takes place by supplying interactive quizzes for you to complete and share with friends!
useful for daily medical emergencies, or even extreme scenarios. By offering step-by-step instructions during any emergency, this app becomes remarkably useful. There are videos and animations that describe in detail ways to provide care until emergency responders are able to take over. This app can also become a way for you to test your first aid skills before an emergency takes place by supplying interactive quizzes for you to complete and share with friends! providing the latest research and so much more. This app allows users to request appointments now, rather than waiting on hold all day. Once the appointment is confirmed, the app then allows users to add this information directly to his or her phone. This app is designed to help users understand more about his health history and any other questions that may arise. While the app has many great features, the ability to share and view lab results at the same pace of your physician is something that is extremely pertinent. This app allows you to view x-rays and MRIs on your phone in a timely manner. It may seem overwhelming for some individuals, but the connectivity of this app is transforming the relationship between physicians and their patients.
providing the latest research and so much more. This app allows users to request appointments now, rather than waiting on hold all day. Once the appointment is confirmed, the app then allows users to add this information directly to his or her phone. This app is designed to help users understand more about his health history and any other questions that may arise. While the app has many great features, the ability to share and view lab results at the same pace of your physician is something that is extremely pertinent. This app allows you to view x-rays and MRIs on your phone in a timely manner. It may seem overwhelming for some individuals, but the connectivity of this app is transforming the relationship between physicians and their patients. This medical app by Webmd is extremely useful for those looking to answer questions about certain symptoms, as well as drug and treatment information. Like the Webmd website, the app is full of detailed information about specific diseases and conditions, as well as the options for treatment. While the basic app is packed with helpful tips and information, Webmd has also developed several other apps specific for your medical condition or current issues.
This medical app by Webmd is extremely useful for those looking to answer questions about certain symptoms, as well as drug and treatment information. Like the Webmd website, the app is full of detailed information about specific diseases and conditions, as well as the options for treatment. While the basic app is packed with helpful tips and information, Webmd has also developed several other apps specific for your medical condition or current issues. In terms of medical apps, Itriage provides a combination of connectivity and knowledge. This app allows users to navigate hospitals and healthcare providers in the area in the event of an emergency. This seems to be extremely useful for families traveling with sick children that may need medical attention quickly. It doesn’t matter if you are unfamiliar to the area, because this app will help you navigate your way to a physician. Don’t forget this app has other features like the ability to research your symptoms, medications and conditions. The app has a built in feature for those in need of certain hotlines as well.
In terms of medical apps, Itriage provides a combination of connectivity and knowledge. This app allows users to navigate hospitals and healthcare providers in the area in the event of an emergency. This seems to be extremely useful for families traveling with sick children that may need medical attention quickly. It doesn’t matter if you are unfamiliar to the area, because this app will help you navigate your way to a physician. Don’t forget this app has other features like the ability to research your symptoms, medications and conditions. The app has a built in feature for those in need of certain hotlines as well.




 and work with the patinets together in the same room. It was so neat to be able to see all different women at different levels of medical education working together to help patients. The whole experience was incredibly empowering, and Dr. Grossfeld has truly inspired me to continue on my own path toward becoming a physician.
and work with the patinets together in the same room. It was so neat to be able to see all different women at different levels of medical education working together to help patients. The whole experience was incredibly empowering, and Dr. Grossfeld has truly inspired me to continue on my own path toward becoming a physician.  ut Bicycle Accidents – 10 Things to Know
ut Bicycle Accidents – 10 Things to Know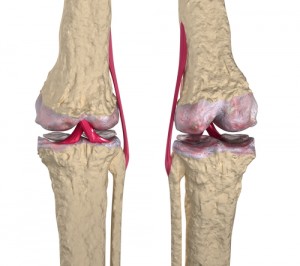

Recent Comments